
What is the correct way of using Medical Service Modifiers for flawless Medical Billing?
When you code for multiple medical services or procedures performed on the same day, a modifier needs to be appended with the said HCPCs or CPT codes in order to get them paid. CMS did a good job in providing a list of modifiers that can be used rightfully to get those claims reimbursed.
However, on the other hand OIG keeps putting up publications and reports on how even the most commonly used modifiers are continuously being abused in various healthcare practices; knowingly and unknowingly.
Inaccurate use of modifiers can lead to:
- Unjustified upcoding
- Documentation loopholes
- Improper payments or overpayments
- Denials
- Raising red flags for fraudulency
- Targeted extensive audits
- Reversals on payments
In this short article we touch upon few of the commonly used modifiers and how we can be compliant to their accurate use.
Modifier 25 Definition: “Significant, separately identifiable evaluation and management (E/M) service by the same physician or other qualified health care professional on the same day of the procedure or other service.”
It is inappropriate to append Modifier 25 when:
Modifier 25 should be used only with the E/M service portion of the claims. Procedures submitted in conjunction with an E/M service do not need modifier 25 in order to be paid. The other procedure should be separately identifiable, as per regulation. Which means the provider must furnish this service only when it’s required to go beyond the level of E/M service they have already provided. This may also lead to addition of separate diagnosis codes as the base of medical necessity. Remember that two different diagnosis codes alone do not justify adding modifier 25. It may be necessary to use the phrase "additional documentation available upon request" in the narrative field of your claim in order to support the modifier used. While you do not need to use two different diagnosis codes, you must document both the E/M service and procedure.
It is inappropriate to append Modifier 25 to:
- Codes other than E/Ms
- Surgical codes
- Medical procedures
- Diagnostic tests
- When no other service(s) was performed
- Post-op services (Especially unrelated to surgery)
- Provider who didn’t perform the service
- Undocumented procedures
Modifier 59 Definition: “Distinct Procedural Service.”
Modifier 59 is one of the most used (and abused) modifiers. Modifier 59 identifies procedures/services that are not normally reported together.
It’s appropriate to append Modifier 59 and its subsets when:
- When there is no other appropriate modifier applicable to disguise the performed services.
- It’s used when there an unrelated service(s) is performed by a same provider on the same day as the office visit.
- It’s appended with same (or similar) procedures which are not usually is performed in the same encounter. Although documentation must support their use on a different session, procedure or surgery, site or organ system, separate incision/excision, separate lesion or injury.
Tip: If documentation supports use modifier 59 or –XS (Separate Structure) for different anatomical sites.
- Modifier 59 or XE can also be appended to distinguish two different unit of intervals of the same service.
- Use modifiers 59 or –XU properly for a diagnostic procedure which is performed before a therapeutic procedure only when the diagnostic procedure is the basis for performing the therapeutic procedure
- Use modifiers 59 or –XU properly for a diagnostic procedure which occurs after a completed therapeutic procedure only when the diagnostic procedure isn’t a common, expected, or necessary follow-up to the therapeutic procedure.
It is inappropriate to append Modifier 59 when:
- Modifier 59 is attached to an E/M service.
- To report a separate and distinct E/M service with a non-E/M service performed on the same date, check to see if modifier 25 is appropriate.
- Just because the code descriptors of the two codes are different.
- In order to unbundle performed procedures by unfair means
Though the National Correct Coding Initiative (NCCI) edits allow the use of modifier 59, determining if it is appropriate to use can be tricky. To read more about bundling and unbundling of multiple procedure payment, visit here:
Modifier 26 Definition: “Professional Component of the services”
Modifier TC Definition: “Technical Component of the services”
These two modifiers are fairly common when billing Diagnostic Radiology services. These usually involve an equipment to perform these services like X-ray, MRI, CT-scan, Ultrasound and more.
A Provider is eligible to bill for TC & 26 Modifier only if they review and interpret the reports in an Office (Non-Facility setting) and most importantly also owns that equipment. If they don’t own the equipment, they only bill services with Modifier 26. However, a Provider can only bill for Professional component while working in a hospital or other Facility settings. Modifier TC is not allowed in these cases as the Hospital has the ownership of the equipment.
- Use TC modifier only for the medical equipment, Facility or the technician. Using only TC modifier indicates only the technical portion of the procedure is used.
- Use 26 modifier for the physician or professional services only. Also, do use them for CPT codes like 93101 with description interpretation and report only.
When both the professional and technical portion is provided by the physician, we are not supposed to use 26 or TC modifier along with CPT code. In such case, the CPT code will be a global code like 73130 only (without any modifiers).
Before using the 26 or TC modifiers, you should check whether the procedure code can accept these modifiers. An indicator of "1" in the PC (Professional Component)/ TC (Technical Component) field on MPFSDB (Medicare Physician Fee Schedule Database) signifies that Modifiers 26 and TC are valid for the procedure code.
Now, how to find out the which CPT code require these Modifiers? Just click below link (at the end of the article), to check the eligibility of CPT code for 26 or TC modifiers.
After visiting the CMS website, you can search for allowed amounts and Facility and Non-Facility Payments. While you may do that you can also confirm if any particular radiology CPT code might need TC or 26 Modifier. We just have to put the CPT code in given search bar and also add the other relevant information and rest is easy:
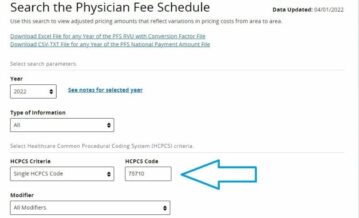

Searching the CPT code will come with the result like shown in the figure. Here we can see that Modifier TC and 26 are indeed applicable with 75710 CPT code here. You may also observe difference the Pricing of the Modifiers here. Which is important to note because they directly impact the payment of the services billed.
Importance of Sequencing Modifiers
Sequencing Modifiers is another important feat to perform to signify the important Modifiers to the payers. It is similar to sequencing Primary Diagnosis code while adding ICD-10 codes in the claims.
When it is necessary to report the following payment modifiers with another modifier, the payment modifier must be reported in the first modifier field. These payment modifiers are not limited to the first position. (If there is another pricing modifier submitted that is required to be in the first modifier field, these modifiers should be in the second, third or fourth modifier position).
The general order of sequencing modifiers is (1) pricing (2) payment (3) location. Location modifiers, in all coding situations, are coded “last”.
For example; If you code two pricing modifiers that include either a professional or technical component (26 or TC), always use the 26 or TC first, followed by the second pricing modifier.
AltuMED PracticeFit enables Medical Billers with an inbuilt scrubber feature, reducing the chances of coding errors to 92%. Schedule a PracticeFit demo to know more:
Subscribe to Our Newsletter!
Subscribe to Our Newsletter!
Enter Your Email Address. We Promise We Won't Spam You