
Understanding Carotid Angiography Bundling Intricacies and Coding Hierarchies - A guide for Medical Billers and Medical Coders
Angiography codes (coronary or non-coronary) quite often leaves a big question mark when it comes to their coding. The possible reasons behind this could be:
a) Reporting codes with their proper hierarchy in mind when vascular system keeps branching-off.
b) Confusing integration of basic procedures like diagnostic imaging (angiography), catheter placement and access (catheterization) or other services performed relevant during an interventional procedure.
If you are new to coding, Cerebral & Carotid Angiography or ‘Cervicocerebral studies’ are simple.
After rassling with the idea of how to accurately report these codes for a while, a number of things started coming into fruition. Even though it could be a little boggling at first however once some effective pointers with road maps are made things would start to make sense and their ‘hierarchy’ will become more profound and easy to understand.
In this article we go through these helpful pointers and share what made coding for such extensive procedures easy for us.
Carotid Angiography
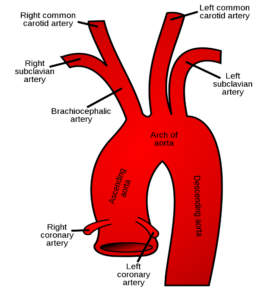
Carotid arteries emerge from Aortic Arch arising from the heart and the supply blood to head, neck and arms. Cerebral angiography is usually a straightforward non-invasive procedure that is performed as an inpatient/outpatient procedure, usually takes about 30–60 minutes to complete. Cerebral angiography is generally performed to study cerebral and carotid arteries to figure out different etiologies for ischemic/hemorrhagic stroke, embolism, aneurysm and many others.
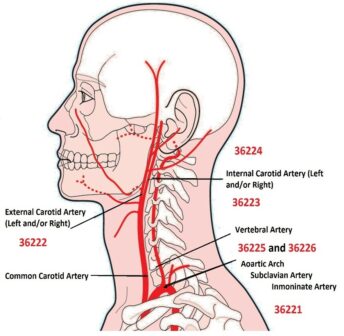
Now, back in 2013, eight new codes were introduced to report differentiated ‘nonselective’ and ‘selective’ arterial catheter placement and diagnostic imaging. The CPT codes ranging for 36221-36228 comprises of the Non-Selective and Selective Catheterization for Cerebral angiogram.
To better understand the coding of these procedures, we need to understand three things to begin with:
First: A little bit of Anatomy of Carotid arterial system (aortic arch, carotid, and vertebral arteries).
Second: Where was the Catheter was located and contrast was injected?
Last: We need to understand, what part of Carotid system was actually Imaged.
Let’s have a look at the codes.
Non-Selective Aortic Arch Angiography:
Staring with the most basic service of the bunch i.e., non-selective aortic arch angiography.
36221 non-selective catheter placements: Thoracic Aorta, with angiography: Extracranial Carotid, Vertebral and/or Intracranial Vessels, unilateral or bilateral, and all associated RS&I, includes angiography of the Cervicocerebral Arch, when performed.
The thing to note here is that although non-selective aortogram can be billed as a stand-alone code (or with other abdominal angiography codes perhaps), it is considered bundled into all the selective codes that follow down below.
Selective Carotid Artery Angiography:
All these codes are for selective unilateral carotid artery imaging. There is a hierarchy of these services based on level of catheter selection and the amount of imaging performed.
Only one of these three codes is applicable per side in the following order: 36224 > 36223 > 32222.
What is included in these codes: Primary Codes 36221-36226 include catheterization, angiography, and radiological supervision and interpretation. There won’t be any need for separate coding for Catheter placement or radiological services.
- Vessel access
- Catheter placement
- Contrast injections
- Fluoroscopic Guidance
- Radiological supervision and interpretation (S&I)
- Arterial closure by pressure or device
Read on to learn details that will help you choose among the different code possibilities.
Again, the focus should be on location of where the catheter was placed and where the imaging was performed. For this we figured out a color-coded system to simplify thing, they are used for Catheter Placement or insertion, the actual angiography or imaging and finally the bundled imaging as a part of the coding hierarchy. We hope it will be easy to follow:
36222 Selective catheter placements: Common Carotid or Innominate Artery, unilateral, any approach, with angiography: Extracranial Carotid circulation and all associated RS&I, includes angiography of the Cervicocerebral Arch, when performed
36223 Selective catheter placements: Common Carotid or Innominate Artery, unilateral, any approach, with angiography: Intracranial Carotid circulation and all associated RS&I, includes angiography of the Extracranial Carotid and Cervicocerebral Arch, when performed
36224 Selective catheter placements: Internal Carotid Artery, unilateral, with angiography: Intracranial Carotid circulation and all associated RS&I, includes angiography of the Extracranial Carotid and Cervicocerebral Arch, when performed
Add-On Code for Angiography:
+36227 Selective catheter placements: External Carotid Artery, External Carotid Circulation and all associated RS&I (List separately in addition to code for primary procedure)
- Use of CPT add-on code 36227 should be reported in conjunction with 36222, 36223, or 36224.
Selective Vertebral Artery Angiography:
Only one of these two codes is applicable per side in the following order: 36226 > 36225.
36225 Selective catheter placements: Subclavian or Innominate Artery, unilateral, with angiography: Vertebral Circulation and all associate RS&I, includes angiography of the Cervicocerebral Arch, when performed
36226 Selective catheter placements: Vertebral Artery, unilateral, with angiography: Vertebral Circulation and all associated RS&I, includes angiography of the Cervicocerebral Arch, when performed
- Use of CPT add-on code 36228 requires use of either CPT code 36224 or 36226.
Add-On Code for Angiography:
+36228 Selective catheter placement, each Intracranial Branch of the internal carotid or vertebral arteries, unilateral, with angiography of the selected vessel circulation and all associated RS&I (i.e., middle cerebral artery, posterior inferior cerebellar artery) (List separately in addition to code for primary procedure).
Some quick tips to wrap it all up!
- Choose the Most Comprehensive Service.
- These codes are hierarchical, meaning these codes are built on a set-up, which determines the lower numbered codes or lesser codes are valued into the higher numbered codes.
- Report only one code from 36222-36224 for each same-side carotid territory.
- Choose code that represents the most selective catheter placement and all of the angiography services performed.
- Bilateral procedures with different hierarchies use modifier -59 on the “lesser” code in this hierarchy. Only requirement here is proper documentation.
- Don’t forget 36221 is the only unilateral code. Rest of the codes have bilateral indication. So, append the LT (Left), RT (Right) or 50 (Bilateral) appropriated to the procedure performed. The bilateral modifier is only used for the exact same procedure/code performed bilaterally.
AltuMED PracticeFit enables Medical Billers with an inbuilt scrubber feature, reducing the chances of coding errors to 92%. Schedule a PracticeFit demo to know more:
Subscribe to Our Newsletter!
Subscribe to Our Newsletter!
Enter Your Email Address. We Promise We Won't Spam You
Relevant Articles
Categories
Informational
Educational
Medical Billing Software
Follow Us